Our Work

Our Approach to Improving and Better Connecting Healthcare
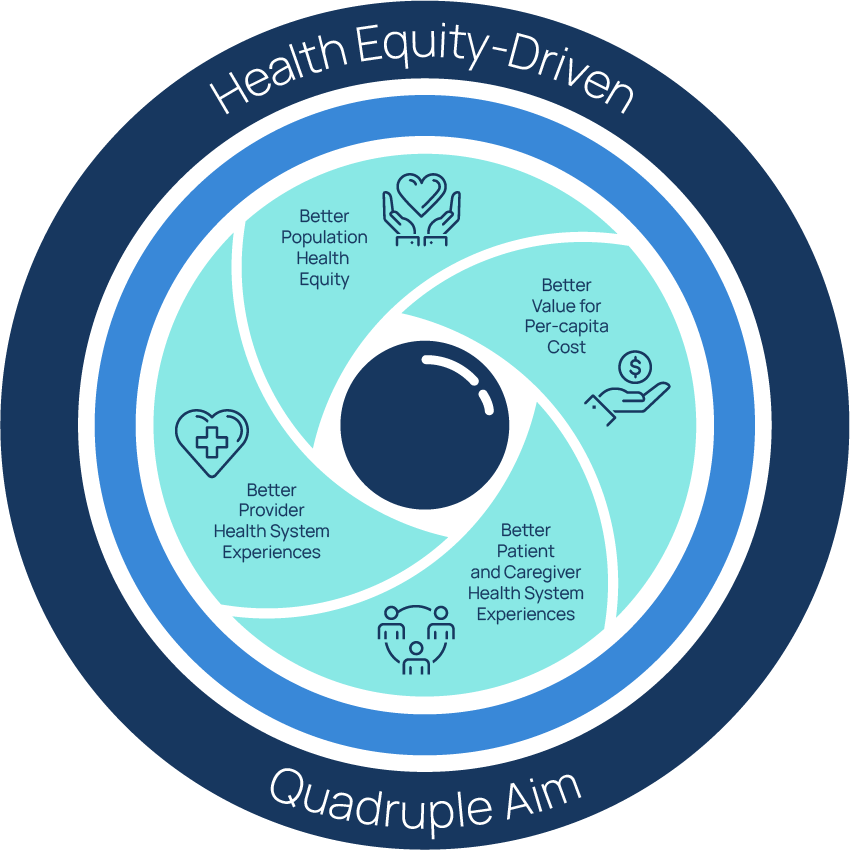
Health Equity-Driven Quadruple Aim
Health equity “allows people to reach their full health potential and receive high-quality care that is fair and appropriate to them and their needs, no matter where they live, what they have, or who they are.”
Health Quality Ontario, 2017
We are committed to a health equity-driven quadruple aim:
- Better population and patient/client health outcomes;
- Better patient/client and caregiver experience;
- Better healthcare provider experience; and
- Better value,
for people living in our community who need these improvements the most.
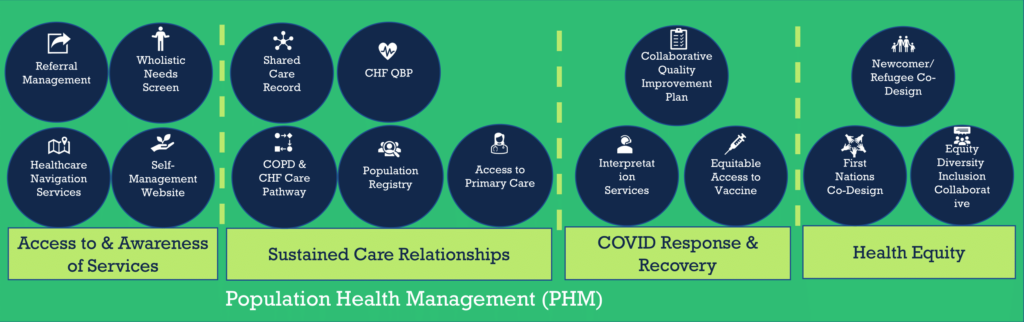
Population Health Management
The Ontario Health Team Coalition for Population Health Management (PHM) endorses the following definition of PHM:
An iterative process which involves gathering data and insights across many partners (including non-traditional healthcare providers) about an entire defined population’s health and social needs. These insights inform the co-design of proactive, integrated, person-centred, cost effective, equitable and efficient solutions with the goal of improving the health outcomes of individuals. (Source: RISE/HSPRN)
The process of Population Health Management includes:
- Population Identification (inclusive of gathering individual population member information to understand the make-up and care needs of the population (may include health and social assessments)*
- Segmentation for needs, risks & barriers
- Co-designing person-centred care models and service mix
- Implementation and reach
- Monitor and Evaluate
(Source: RISE with one modification from Population Health Alliance and California’s Department of Health Care Services*) We understand:
- These definitions to be inclusive of the principles of Health Equity and the Quadruple Aim
- Any reference to ‘Population’ in an OHT context to be reference to our Full Attributed Population
Initial Population of Priority
The Middlesex London OHT will initially focus on improving healthcare and supports for 2,000-3,000 people living with advanced Chronic Obstructive Pulmonary Disease (COPD) and/or Congestive Heart Failure (CHF), who need system-level care coordination or navigation and are at highest risk of hospitalization.
Eventually we will support a population of over 525,000 people with their healthcare needs.

Media Releases

Ontario Health Teams bring HealthPathways to Canada – November 26, 2024